Call Girls Agra Just Call 8250077686 Top Class Call Girl Service Available
Cleft Palate Lip Bifid uvula submucosal cleft modified by Dr Nayyar.ppt
1. 1
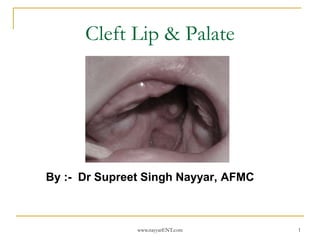
Cleft Lip & Palate
By :- Dr Supreet Singh Nayyar, AFMC
www.nayyarENT.com
2. Bifid uvula
A bifid or bifurcated uvula is a split or cleft uvula.
Newborns with cleft palate also have a split uvula. The
bifid uvula results from incomplete fusion of the palatine
shelves. Bifid uvulas have less muscle in them than a
normal uvula, which may cause recurring problems with
middle ear infections. While swallowing, the soft palate is
pushed backwards, preventing food and drink from
entering the nasal cavity. If the soft palate cannot touch
the back of the throat while swallowing, food and drink
can enter the nasal cavity.[6] Splitting of the uvula occurs
infrequently but is the most common form of mouth and
nose area cleavage among newborns. Bifid uvula occurs
in about 2% of the general population,[7] although some
populations may have a high incidence, such as Native
Americans who have a 10% rate.[8]
Bifid uvula is a common symptom of the rare genetic
syndrome Loeys-Dietz syndrome,[9] which is associated
with an increased risk of aortic aneurysm.[10]
2
www.nayyarENT.com
3. • Submucosal Cleft: A submucosal cleft is a cleft
that is under the mucosa that lines the roof of
the mouth, hence the term “sub.” Because a
submucosal cleft is under the mucosa, the only
physical indicator of its presence may be a bifid
uvula. Even though not seen from the surface,
the muscles of the palate are not joined at the
midline in a submucosal cleft. This creates an
inability to move the palate for some speech
sounds. Hence, a submucosal cleft is usually
diagnosed when a child has abnormal speech
development and a bifid uvula is present.
3
www.nayyarENT.com
5. 5
Introduction
Orofacial clefting is the second most common
congenital deformity (after clubfoot).
Cleft has detrimental effects on speech,
appearance, swallowing, dental, hearing,
facial growth, emotions
Multidisciplinary team approach
Time consuming, multistage treatment
www.nayyarENT.com
6. 6
Epidemiology
Incidence of Orofacial clefting: 1:700 live births
68% to 86% of cleft palate is associated with
cleft lip
Isolated cleft palate- more in females
Cleft lip (with or without cleft palate)- more in
males
Unilateral CL(P) is more common, more on left
side
www.nayyarENT.com
7. 7
Embryology
palate forms through the fusion of two paired
outgrowths of the maxillary prominences, the
palatal shelves.
palatal shelves appear during the 6th week of
development
during the 7th week, the shelves elevate,
assume a horizontal orientation, and fuse.
www.nayyarENT.com
8. 8
Embryology
fusion begins at the incisive
foramen, progresses toward the
posterior palate, and is complete at
about the 12th week of intrauterine
life.
Cleft palate – failure of fusion of
palatal shelves
Intrauterine development of secondary palate, 6 weeks to 12 weeks.
www.nayyarENT.com
9. 9
Anatomy-Bones of the Palate
Premaxilla
Paired maxilla
Paired palatal bones
www.nayyarENT.com
10. 10
Anatomy-Muscles of the Palate
Extrinsic muscles
Levator veli palatini
Tensor veli palatini
Palatopharyngeus
Palatoglossus
Salpingopharyngeus
Superior constrictor
Intrinsic muscle
Musculus uvulae
www.nayyarENT.com
11. 11
Levator veli palatini
Origin: posteromedial
Eustachian Tube
Insertion: palatal
midline
Function: elevates soft
palate: ET dilatation
In cleft palate:
hypoplastic and thin.
www.nayyarENT.com
12. 12
Tensor veli palatini
Origin: scaphoid fossa of sphenoid
Insertion: aponeurosis on the posterior hard palate
Function: Eustachian Tube dilatation
In cleft palate: lesser numbers of fibres
www.nayyarENT.com
13. 13
Palatopharyngeus
Origin: posterior border of aponeurosis and
levator
Insertion: lateral pharynx and larynx
Function: antagonistic to levator: helps in
velopharyngeal closure
www.nayyarENT.com
14. 15
Musculus Uvulae
Origin: anterior to the
aponeurosis in the midline
Insertion: posterior
connective tissue of the
midline
Function: velopharyngeal
closure
In cleft palate:
www.nayyarENT.com
15. 16
Causes - Mechanical Causes
i) palatal shelves hypoplasia
ii) increased resistance to palatal
shelves
iii) excessive head width
iv) failure of shelf fusion
www.nayyarENT.com
16. 17
Causes - Genetic causes
defect in genetic loci
TGF alfa,
TGF beta3,
T-BOX 22,
P-63,
procollagen type XI
www.nayyarENT.com
18. 19
Symptoms
Separation of the lip
Separation of the
palate
Nasal distortion
Recurring ear infections
Hearing loss
www.nayyarENT.com
19. 20
Symptoms (cont.)
Failure to gain weight
Nasal regurgitation
when bottle feeding
Poor speech
Misaligned teeth
Growth retardation
www.nayyarENT.com
20. 21
Classification of Cleft Palate
Several classification system based on
morphology, anatomy & embryologic
development
Davis & Ritchie (morphological classification)
Basis of involvement of alveolar process
Gr I: Prealveolar cleft
Gr II: Postalveolar clefts
Gr III: Alveolar clefts
www.nayyarENT.com
21. 22
Classification of Cleft Palate
Veau’s classifications(1931):
Gr I: Cleft of soft palate
Gr II: Cleft of soft & hard palate
Gr III: Complete unilateral cleft
Gr IV: Complete bilateral cleft
www.nayyarENT.com
22. 23
Classification of Cleft Palate
Kernahan & Stark classification(1958):
Based on embryologic development
www.nayyarENT.com
23. 24
Classification of Cleft Palate
Kernahan symbolic (Y) classification:
Elsahy modification of Y classification:
www.nayyarENT.com
24. 25
Classification of Cleft Palate
Kriens classification:
‘LAHSHAL’ code based on anatomy
www.nayyarENT.com
25. 26
Management principles
Assessment & identification of associated
anomalies
* Birth history
* Examination of Head & Neck
* Nasal endoscopy
* Otolaryngologic assessment
Associated problems of feeding, speech
Parental counseling
www.nayyarENT.com
26. 27
Management principles
Feeding:
Immediate concern
Special feeding bottles
* Squeeze bottles
* Haberman bottle
Care needed to burp
the child after each
feed
www.nayyarENT.com
27. 28
Orthodontic manipulation
Required for cleft of primary palate
Alignment of alveolar arch required before
surgical intervention
eg McNeil, Burston method
www.nayyarENT.com
28. 29
Cleft palate repair - History
Chin (Tsin) Dynasty, Circa 390AD
Cleft palate confused with oronasal fistula
of tertiary syphilis
Philibert Roux (1819)
Dieffenbach’s (1840)
Von Langenbeck
www.nayyarENT.com
30. 31
Cleft palate repair
Goals of cleft palate repair
* separate oral & nasal cavity
* normalize swallowing
* normalize speech- help of speech therapy
* limit side effect of cleft palate repair-
defective midfacial growth
* prevent tooth loss by alveolar bone graft
www.nayyarENT.com
31. 32
Timing of cleft palate repair
Speech outcome
Maxillary growth
Syndromic child with cleft palate
Lip repair – 6 wks to 12 wks
Palate repair – 10 to 12 mths
www.nayyarENT.com
32. 33
Techniques of Palatal repair
Von Langenbeck Technique
* uses mucoperiosteal flap
to close defect in sec palate
* old method still used
www.nayyarENT.com
33. 34
Von Langenbeck (cont..)
Adv:
• Can be used for ant palatal repair
Disadv:
• Not suitable for wide defect
• Does not increase velar length
• Shortens growing maxilla
www.nayyarENT.com
36. Surgical Repair- Cleft Lip
Cleft lip repaired at 10
weeks
Rotation-advancement
method- Most common
Nine Landmarks
Rotation Flap cuts
made first
Advancement cuts
made next
Cleft side nasal ala cuts
made last
www.nayyarENT.com 37
37. 38
Push back Technique
Adv:
* Can be used for wide cleft defect
* Address the velopharyngeal incompetence
Disadv:
• Cannot address the anterior cleft defect
• Narrow dev of ant alveolar arch
• Limits palatal lengthening
www.nayyarENT.com
39. 40
Furlow Z-plasty
Adv:
• Lengthening of velum
• Recreates levator sling
• Hard palate can also be addressed
Disadv:
• Increased operative time
• Technically difficult
www.nayyarENT.com
41. 42
Patient support - Speech therapy
Because of surgery
being done so early
hopefully speech will
form correctly but
because the child has
to adapt, therapy is
advised.
www.nayyarENT.com
42. 43
Patient support - orthodontics
as the child gets older
teeth are not straight -
orthodontist for
treatment (braces).
www.nayyarENT.com
43. 44
Conclusions
Cleft Palate are common congenital
deformities that often affect speech, hearing,
and cosmesis; and may at times lead to
airway compromise.
The otolaryngologist is a key member of the
cleft palate team, and is in a unique position
to identify and manage many of these
problems .
www.nayyarENT.com
44. 45
References
Pediatric Plastic Surgery,Mathes,2nd edition,
Vol IV.
Otolaryngologic Clinics of North America,
2007
Scott- Brown’s Otolaryngology, 6th & 7th
edition.
www.nayyarENT.com
45. 46
Further Information
Cleft Palate Foundation
www.cleftline.org
Cleft Lip and Palate Association CLAPA
www.clapa.com
Online support group
www.cleftclub.com
www.nayyarENT.com
![ Bifid uvula
A bifid or bifurcated uvula is a split or cleft uvula.
Newborns with cleft palate also have a split uvula. The
bifid uvula results from incomplete fusion of the palatine
shelves. Bifid uvulas have less muscle in them than a
normal uvula, which may cause recurring problems with
middle ear infections. While swallowing, the soft palate is
pushed backwards, preventing food and drink from
entering the nasal cavity. If the soft palate cannot touch
the back of the throat while swallowing, food and drink
can enter the nasal cavity.[6] Splitting of the uvula occurs
infrequently but is the most common form of mouth and
nose area cleavage among newborns. Bifid uvula occurs
in about 2% of the general population,[7] although some
populations may have a high incidence, such as Native
Americans who have a 10% rate.[8]
Bifid uvula is a common symptom of the rare genetic
syndrome Loeys-Dietz syndrome,[9] which is associated
with an increased risk of aortic aneurysm.[10]
2
www.nayyarENT.com](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)