Overview
Nail bed injuries are considered trivial by many people, so treatment is often delayed. However, optimal initial management of the damaged nail bed decreases the likelihood of chronic painful nail plate deformity.
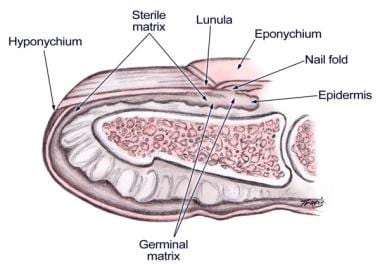
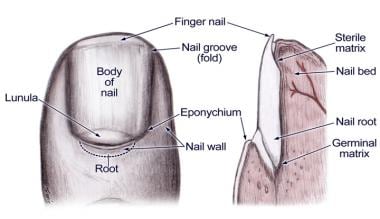
The images below depict nailbed anatomy.
Injuries of the nail bed most commonly result from compression of the nail bed between the bent or broken nail and the distal phalanx of the finger; this compression is usually due to localized trauma. [1] Stellate laceration or multiple fragments of nail bed can occur when the nail is crushed between a larger object and the bone. A sharp object often goes through the nail and amputates the tip rather than stopping; this causes a clean laceration of nail bed. The middle and distal thirds of the nail bed are the most frequent sites of injury, and 50% of injuries involve fracture of the distal phalanx, tuft, or both.
Primary assessment includes obtaining a good patient history, including the timing and mechanism of the injury. The physical examination should looks for signs of contamination, exposure of bone, viability of surrounding skin, and evidence of fingertip contusion. Radiographs may be helpful in evaluating for the level and extent of bony injury.
Indications
Treatment of the following acute injuries, in decreasing order of incidence [2] :
-
Simple lacerations (most common injury)
-
Stellate lacerations
-
Severe crush injury
-
Avulsion of the nail from the nail fold perionychium [3]
-
Subungual hematoma [4, 5] involving over 25-50% of the visible nail
Contraindications
No absolute contraindications exist. Late reconstruction procedures of the nail bed are commonly not as successful as the surgeon or the patient desires.
Anesthesia
The following anesthetic procedures are commonly used for hand and nail bed repair:
-
Local ring block
-
Regional/digital block (if associated proximal injuries require some intervention)
-
Procedural sedation (typically only needed for young children)
Equipment
See the list below:
-
Surgical preparatory supplies
-
Finger tourniquet
-
Iris scissors or small Kutz periosteal elevator
-
Povidone iodine (eg, Betadine) solution
-
Loupe magnification, if needed
-
Removed nail (preferred) or Silastic sheet
-
Sutures, 6-0 or 7-0 absorbable monofilament suture material and 6-0 nylon
-
Nonadherent gauze
Positioning
Position the patient supine.
Abduct the arm.
Place the hand on an arm extension with the forearm/palm prone.
The image below depicts positioning of the finger.

Technique
After surgical preparation of the site, apply a finger tourniquet to allow a bloodless view of the nail bed.
Insert the blades of curved Iris scissors or a small periosteal elevator beneath the free edge of the nail (hyponychium). Gently open and close the Iris scissors blades or gently press the nail bed with the small periosteal elevator, taking care to minimize trauma to the nail bed. Advance proximally in between the nail plate and the nail bed until the instrument reaches the nail fold.
After the nail is removed, scrape the residual soft tissue from its undersurface and then soak it in povidone iodine solution while the nail bed is being repaired.
Simple lacerations
When a subungual hematoma exists with an intact nail, an underlying simple laceration may be present. If the laceration does not extend beyond the lateral nail fold and if no significant deformity or fracture of the nail is present, the nail should not generally be removed to rule out laceration. In this situation, the laceration is more likely to heal well without nail removal and laceration repair. Instead, nail trephination alone can be performed to evacuate the subungual hematoma. See the image below.

Explore the nail bed under loupe magnification (if necessary).
Trim the irregularities so that the tissue can be repaired without any tension on closing.
For accurate wound approximation, undermine one millimeter of the nail bed from the periosteum (this allows slight eversion of the wound edges).
After the nail bed is accurately approximated, suture the margins of the laceration with 6-0 or 7-0 absorbable monofilament sutures.
Drill a round hole or burn through the nail plate at a point not over the repair site to allow drainage of serum or hematoma from the subungual area after the nail is reinserted into the nail fold (the nail keeps the fold open and better molds the edges of the repair).
Hold the nail in place with Steri-Strips or a 6-0 monofilament nylon suture placed either through the fingertip and the distal free border of the nail plate or through the lateral nail folds and nail plate. Another option is a dorsal figure-of-eight suture. To achieve this stitch, place a suture transversely just distal to the hyponychium, then take another bite proximal to the nail fold in the same direction and tie it back to the initial stitch location.
Apply nonadherent dressings and a splint that immobilizes the distal interphalangeal joint and protects the tip.
The dressing needs to be changed in 5-7 days and the nail checked for subungual seroma or hematoma.
The suture should be removed from the tip at 2-3 weeks.
The nail frequently adheres to the nail bed for 1-3 months until pushed off by the new nail.
Replacement of the nail creates a much less tender fingertip while a new nail is growing. However, not placing the nail plate back into the nail fold is also an option.
Complex stellate lacerations
In severe crush injuries, any fragment attached by tissue strands should be accurately replaced if not severely devitalized.
Any small segments of nail bed attached to the detached nail should be removed with a small periosteal elevator and used as free grafts to complete the nail bed repair.
Avulsed nail bed
In avulsion of the nail bed with the nail, the nail should be replaced accurately without attempting to separate the nail and nail bed to avoid further injuries to the nail bed.
Distal phalanx fracture
In lacerations associated with fractures of the distal phalanx, if the fracture is nondisplaced, the nail bed should be repaired and the nail replaced as a splint.
The displaced fractures of the distal phalanx should be reduced evenly before the nail bed is repaired, as the nail bed deformity will result if the dorsal cortex of the distal phalanx is left uneven.
Missing nail plate
If the nail plate is unavailable or too badly damaged for a portion of it to be replaced (see the image below), a nail-shaped sheet of reinforced silicone or a sterile petroleum gauze may be placed as a sterile dressing within the nail fold as a substitute after nail bed repair.

Pearls
Trephination alone without nail removal and laceration repair may be adequate in the setting of a subungual hematoma with an intact nail plate.
Some suggest elevating and retracting the nail plate rather than removing it completely to facilitate the nail bed repair.
All retrievable fragments of nail bed should be replaced as free grafts. A graft of 1 cm in diameter will usually live by inosculation and ingrowth of circulation from the periphery, even on the bare cortex of the distal phalanx.
The nail plate can be repaired using tissue adhesives such as Indermil (n-butyl cyanoacrylate) or Histoacryl (2-butyl-cyanoacrylate), which contain no toxicological hazard. [6, 7] The same glue can be used instead of a stitch to secure the nail to nail bed and hyponychium.
Complications
See the list below:
-
Infection
-
Bleeding
-
Nonadherence
-
Ridging
-
Split nail
-
Absent nail growth
-
Nail spikes
Questions & Answers
Overview
What are indications for nail bed laceration repair?
What are contraindications for nail bed laceration repair?
How is anesthesia administered in nail bed laceration repair?
Which equipment is needed for nail bed laceration repair?
What is the proper patient positioning for nail bed laceration repair?
How is nail bed laceration repair performed?
What is the procedure for nail bed repair of simple lacerations?
What is the procedure for nail bed repair of complex stellate lacerations?
What is the procedure for avulsed nail bed repair?
What is the procedure for nail bed repair of distal phalanx fractures?
What is the procedure for a missing nail plate repair?
What are pearls for nail bed laceration repair?
What are potential complications of nail bed laceration repair?
-
Positioning of finger.
-
Nail bed anatomy.
-
Nail bed anatomy.
-
Trephination of a subungual hematoma.
-
Nail bed repair.








